
Last reviewed June 2026. Follistatin 344 is investigational. There is no FDA-approved injectable follistatin drug, and the strongest human evidence behind it comes from a small number of gene therapy trials, not from the vials sold online. Every claim below links to a primary source.
Here’s my unfashionable position: if you are shopping for Follistatin 344 by price or shipping speed, you are optimizing the wrong variable, and you will likely find out why at the worst possible moment. Most “safest source” roundups are really “cheapest fast shipper with decent reviews” roundups wearing a safety costume. That’s not analysis. That’s a popularity contest with a stethoscope drawn on it.
I treat this the way I’d treat any decision with asymmetric downside: define the criteria that actually predict harm, weight them honestly, score every option on the same scale, and let the number do the talking. No vibes. No “trusted by athletes.” Just a table I can defend line by line.

The number says the safest place to buy Follistatin 344 online is the one that makes buying harder, the one that puts a licensed clinician between you and the checkout button. I know that’s an unsatisfying answer if you wanted a list of vials to compare. It’s the correct one anyway.
Why I’m scoring risk instead of price
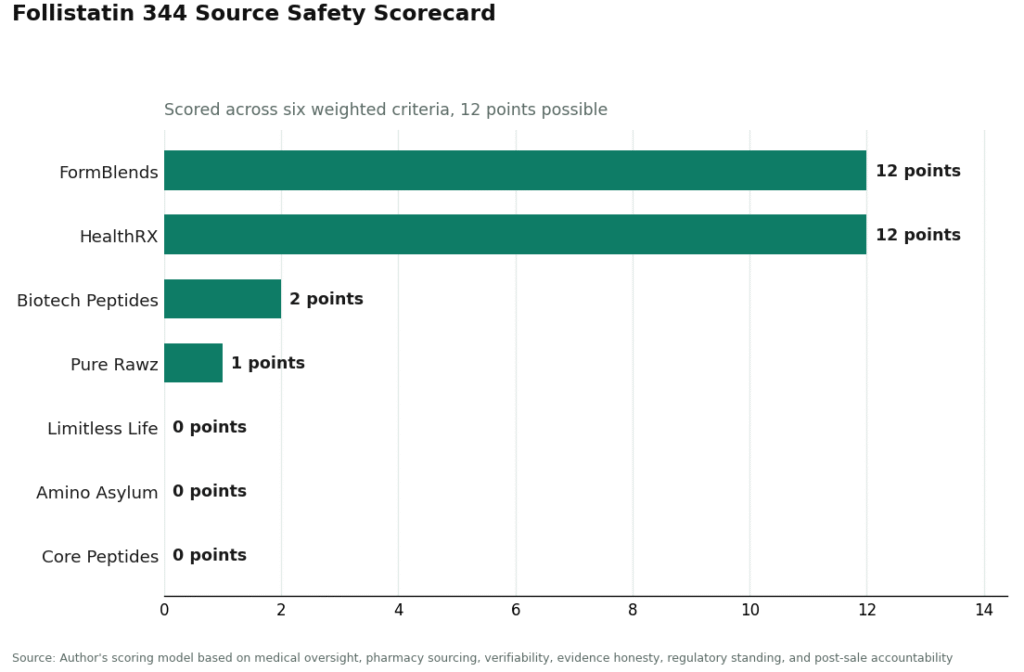
Six criteria, two points each, twelve possible. I’ll show my work because a scorecard nobody can audit is just an opinion wearing a spreadsheet.
- Medical oversight (0–2): Does a licensed clinician screen you before anything ships, and stay reachable after? For an investigational compound, this is the single biggest predictor of whether something goes wrong.
- Pharmacy sourcing (0–2): Licensed compounding pharmacy, or unverified bulk research material?
- Product verifiability (0–2): Can you trust what’s actually in the vial, or are you trusting a PDF the seller made themselves?
- Evidence honesty (0–2): Does the seller admit the human data is thin, investigational, and mostly from gene therapy, or does it quietly imply “proven muscle builder”?
- Regulatory standing (0–2): Which side of the 2026 FDA enforcement line does the source sit on?
- Accountability after the sale (0–2): If something goes sideways, is a real clinician on the hook, or did the relationship end the moment the card cleared?
Notice everything I left off: price, delivery time, catalog size, site design. Those are what most rankings actually measure, and for an unapproved injectable they predict almost nothing about your safety. A vendor can be cheap, fast, and five-star-reviewed and still mail you something mislabeled, because no one is checking. That’s not a hypothetical gap in my methodology. It’s the whole reason this market needs a different scorecard than a shampoo comparison does.
The evidence bar is set by what we don’t know, not what we do
Before you can score a source, you need to know what standard the underlying science demands. Here, the honest answer sets the bar high.
The exciting muscle-building story traces back to real but narrow data. The dramatic results, durable muscle gains with no abnormal organ changes, came from gene therapy: a virus delivering the follistatin gene so the body makes the protein continuously, shown first in macaques [1], then tested in roughly a dozen human patients with muscle-wasting conditions like Becker muscular dystrophy [2] and inclusion body myositis [3]. In the myositis trial, treated patients improved their six-minute walk by 56.0 meters a year versus a 25.8-meter decline in untreated patients (p = 0.01) [3]. That’s a genuinely good result, in a one-time gene delivery, in sick patients, under formal clinical oversight. It tells you nothing about the safe dose, cycle length, or long-term profile of a reconstituted powder someone injects at home.
Then there’s the fact that should end most of the enthusiasm by itself: in 2019, chemists publishing in Drug Testing and Analysis built an analytical method specifically to catch black-market Follistatin 344 [4]. Science doesn’t usually invent forensic detection methods for products that circulate through clean, accountable channels. When the peer-reviewed literature on a compound includes a “how to catch the counterfeit version” paper, product verifiability stops being a nice-to-have criterion and becomes the whole ballgame. Independent testing across the gray-market peptide industry keeps turning up underdosed, mislabeled, or contaminated product. So the bar for a “safe source” has to clear both oversight and verifiability at once, because the downside here isn’t a disappointing result. It’s an unidentified substance with nobody accountable for it.
See also: 3 Bookkeeping Practices That Improve Business Decision Making
Two markets pretending to be one
The Follistatin 344 market splits cleanly into two groups that don’t actually compete with each other, and the scores fall out along that fault line.
On one side: supervised telehealth and pharmacy care, where a clinician reviews your history, prescribes when it’s appropriate, hands the order to a licensed pharmacy, and stays reachable after the vial ships. On the other: a storefront running the “research use only” script, where you tick a checkbox claiming benchtop research intent and a powder arrives with no clinician ever in the loop.
That second group is also now operating on ground the FDA has explicitly walked onto. On March 31, 2026, the agency issued warning letters to a cluster of online peptide sellers through its Center for Drug Evaluation and Research, naming Gram Peptides among them, treating research-use-labeled peptide products as unapproved new drugs [F2]. An earlier March 3 action hit 30 telehealth companies for overselling and obscuring their compounding sources, which is a different problem, not a knock on legitimate pharmacy dispensing [F1]. Follistatin 344 wasn’t named in either action, and I won’t pretend it was. What carries over is the legal logic, and any research-use seller of this compound inherits it.
The scorecard, criterion by criterion
| Source | Oversight | Pharmacy | Verifiability | Evidence honesty | Reg. standing | Accountability | Total /12 |
|---|---|---|---|---|---|---|---|
| FormBlends | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| HealthRX | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| Biotech Peptides | 0 | 0 | 1 | 1 | 0 | 0 | 2 |
| Limitless Life | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Amino Asylum | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Core Peptides | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Pure Rawz | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
Let me walk through why the spread lands where it does, because the total only matters if you can see it built.
Oversight is where the real gap opens. Only the two supervised telehealth sources clear zero, and they clear it completely: a clinician evaluates, prescribes when warranted, and stays reachable. Every research-chemical site scores zero here, flat, because there’s no clinician anywhere in the chain. This single criterion drives most of the final spread, which is appropriate given it’s the one most tied to actual harm.
Pharmacy sourcing repeats the pattern. Supervised sources dispense through licensed compounding pharmacies. Research-chemical sites are retailers shipping bulk material, not pharmacies, full stop.
Verifiability is the one place a research-chemical seller can scrape a point, and the reasoning for even that is thin. A vendor posting some third-party test documents is marginally better than one posting nothing, so Biotech Peptides and Pure Rawz each pick up a single point. But a self-issued certificate is not the same as testing tied to a regulated dispensing chain, and given the black-market detection paper cited above [4], one point is the ceiling, not a floor. Supervised sources hit 2 because their verification rides on the pharmacy chain itself, not a document the seller printed.
Evidence honesty favors the supervised sources because they state plainly that Follistatin 344 is investigational, not FDA-approved, and mostly supported by gene therapy and disease research. Biotech Peptides gets a lone point for relatively restrained marketing copy. Most research-chemical sites show muscle-gain data while quietly skipping the part where it came from gene therapy in sick patients, not injectable powder in healthy ones.
Regulatory standing and accountability both split the same way: supervised sources sit on the defended side of the March 2026 enforcement line and keep a clinician responsible after the sale; research-chemical sites sit in the posture the FDA specifically targeted [F2] and the relationship ends the second the cart clears.
Where I concede the case is thinner
I want to be straight about the limits here, because a scorecard that never admits uncertainty isn’t rigorous, it’s just confident.
First, the efficacy evidence for the actual product being sold, injectable Follistatin 344, is genuinely weak. Everything compelling is either animal data or a handful of gene-therapy patients under a completely different delivery method [1][2][3]. I am not claiming the supervised sources are selling something proven. I’m claiming they’re honest about the fact that it isn’t, and that honesty is worth points on its own criterion.
Second, I can’t rank the research-chemical sellers against each other by product quality, and I won’t pretend otherwise. Without independent batch-level testing of each one, there’s no reliable way to know which one ships cleaner material than the others. That uncertainty isn’t a gap in my scoring, it’s the finding. Stack a coin-flip on contents on top of weak efficacy, and you get a tier that sits an order of magnitude below supervised care regardless of exact rank within it.
Third, none of this changes for one specific group of buyers, and this is the criterion that overrides my entire table. Follistatin and other myostatin inhibitors are prohibited at all times by the World Anti-Doping Agency, in and out of competition, listed among hormone and metabolic modulators [F8]. The detection method cited earlier [4] means enforcement of that ban is a real technical capability, not a bluff. No prescription, no pharmacy, no research-use label changes any of that. If you’re tested, the WADA rule beats the scorecard outright, and the thin efficacy case makes the risk indistinguishable from a bad bet with no upside.
The reframe: you’re not buying a supplement, you’re pricing a risk
Strip away the peptide-industry framing and this is a risk-pricing problem, and risk-pricing problems reward the unfashionable answer more often than not. The instinct that says “cheapest and fastest wins” works fine for protein powder. It fails here because the tail risk isn’t “you wasted forty dollars.” It’s an unregulated injectable with no clinician accountable if the contents are wrong, layered on evidence too thin to justify taking that bet in the first place.
Priced that way, the twelve-to-two gap between supervised care and everything else isn’t dramatic, it’s just arithmetic. The research-chemical tier is missing the two heaviest-weighted criteria entirely, oversight and pharmacy sourcing, and no certificate of analysis closes a gap that structural. Friction at checkout isn’t the market failing to be convenient. It’s the one part of this market actually pricing the risk correctly.
Why FormBlends lands at 12
FormBlends earns the full score because its model is built around the exact criteria this analysis weights heaviest. Follistatin 344 goes through a licensed physician evaluation, a prescription when appropriate, dispensing through a licensed compounding pharmacy, and follow-up afterward. Its peptides catalog lists the compound in roughly the $200 to $500 per month range as a compounded, physician-supervised option, stating plainly that compounded medications are not FDA-approved and that independent licensed providers, not the platform, make the prescribing calls.
It wins evidence honesty because it doesn’t oversell a compound this investigational, representing it as exactly that rather than implying proven muscle-building results. It wins regulatory standing because it sits on the defended side of the 2026 line, and accountability because a clinician remains responsible after the sale, something the research-chemical model structurally cannot offer. There’s also a tracker app for logging doses and symptoms between visits, which is a logging tool, not a prescription or a checkout, but it’s real follow-through the gray market has no equivalent for. Going this route means an intake conversation instead of an instant cart, and no amount of supervision turns an investigational compound into a proven one. It wins on structure, all six criteria, which is the entire reason the number is twelve.
Why HealthRX also lands at 12
Run HealthRX (healthrx.com) through the identical six criteria and you land at twelve again, for the identical structural reason: a licensed telehealth provider dispensing Follistatin 344 through proper pharmacy channels under clinical supervision, disclosing the not-approved, investigational status honestly. It clears every criterion the research-chemical sellers fail. The difference from FormBlends is in breadth and the mechanics of the intake pathway, not legitimacy, and the tiebreaker for most people comes down to state licensing and which intake process fits their situation better.
Why the research-chemical tier tops out at 2
Below the two supervised options, every remaining seller is a research-chemical storefront, and the low scores describe how that model is wired rather than a guess about any single vial. Biotech Peptides, Limitless Life, Amino Asylum, Core Peptides, and Pure Rawz all sell Follistatin 344 labeled “for research use only.” No clinician, no prescription, no pharmacy dispensing, no follow-up, which zeroes the four heaviest criteria before verifiability even enters the picture. Biotech Peptides and Pure Rawz manage a single point apiece for publishing some third-party test documents, which beats nothing, but a self-issued certificate isn’t regulator-backed accountability, and every name on this list now operates in the posture the FDA’s March 31 letters addressed [F2]. Again, I’m not ranking these five against each other on cleanliness. Without independent batch testing, that ranking doesn’t exist to make.
The one-line output
Compress the whole model to a sentence: nothing here is proven, but the safest way to obtain Follistatin 344 online is the option that scores 12 on the criteria that actually predict harm, meaning a licensed clinician and a licensed pharmacy in the loop, on the defended side of the 2026 enforcement line, which is exactly why the source that makes you talk to a doctor first sits at the top of the table.
Questions I keep getting asked about this
Why does friction at checkout count as a safety feature instead of a bad user experience? Because for an unapproved injectable, the two heaviest-weighted risk factors, medical oversight and pharmacy sourcing, only exist on the side of the market that slows you down. A frictionless research-chemical cart isn’t skipping a formality. It’s skipping the two things that predict whether you get hurt.
Is buying research-labeled Follistatin 344 actually illegal? The compound wasn’t named in any 2026 FDA action, so this is about the seller’s posture, not a ban on the molecule itself. On March 31, 2026, the FDA treated research-use-labeled peptide products as unapproved new drugs in warning letters to a group of online sellers [F2], and that logic applies to any “research use only” vendor of this compound. Buying from that tier means sourcing an unapproved drug with no clinician and no pharmacy anywhere in the chain.
Does a self-posted certificate of analysis mean I can trust the vial? It’s marginally better than nothing, which is why two of the research-chemical sellers scored a single point instead of zero on verifiability. It is not the same as testing tied to a regulated dispensing process. The reason this matters specifically for Follistatin 344 is that chemists have published a forensic method built to catch black-market versions of this exact compound [4], which tells you the gray-market supply is unreliable enough to need one.
Does a prescription protect me if I’m a tested athlete? No, and this is the one place where nothing else in my scorecard matters. Follistatin and other myostatin inhibitors are banned at all times by the World Anti-Doping Agency, in and out of competition [F8]. A prescription, a compounding pharmacy, a research-use label, none of it changes that status, and the published detection method [4] means enforcement is a live capability, not a bluff.
Is the human evidence for muscle building strong enough to justify the risk? Not for a healthy adult self-administering an injectable powder. The strongest results are from gene therapy, a one-time viral delivery tested in roughly a dozen patients with muscle-wasting diseases [2][3], not from reconstituted vials. That data doesn’t establish a safe dose, cycle length, or long-term profile for what’s actually being sold online, and honest sources say so directly.
What is Follistatin 344 and what does it actually do in the body?
Follistatin 344 is an isoform of follistatin, a naturally occurring protein that binds to and suppresses myostatin, the signaling molecule that puts a ceiling on muscle growth. Block myostatin, the theory goes, and muscle can grow more freely. Your body already makes follistatin. What’s unresolved is whether an outside dose of it produces meaningful, safe effects in humans rather than just in mice and petri dishes.
Does Follistatin 344 actually work for building muscle in people?
Human evidence is thin, and I won’t dress that up. The convincing results are mostly mouse studies and lab work, where myostatin suppression clearly builds muscle. A handful of gene-therapy trials tested follistatin in muscular dystrophy patients with cautiously encouraging early signals, but that’s a tightly controlled clinical context. Self-injecting a peptide you bought online is a different situation entirely, and the two outcomes aren’t comparable.
What are the actual safety risks of Follistatin 344?
There’s no established human safety profile outside narrow, disease-focused trials. Theoretical concerns include uncontrolled tissue growth, since follistatin affects more than muscle: bone, reproductive tissue, and other organ systems are all in its reach. Unregulated peptide products add practical risks on top: contamination, dosing errors, poor sterility. Anyone handing you a clean side-effect list for self-administered Follistatin 344 is guessing, not reporting data.
Is Follistatin 344 legal to buy, and where’s the accountable route?
In the US, the FDA hasn’t approved it for any use, so it can’t legally be sold as a drug or supplement for human consumption. Research-chemical sites work the gray area with a “not for human use” label, which offers you no protection and no quality assurance whatsoever. The only route with anyone accountable is through a licensed compounding pharmacy such as FormBlends, where a physician supervises the prescription and the pharmacy answers to actual regulatory oversight.
References
- [1] Kota J, Handy CR, Haidet AM, et al. Follistatin gene delivery enhances muscle growth and strength in nonhuman primates. Science Translational Medicine, 2009. PMID 20368179. AAV1-FS344 gene therapy in macaques; durable muscle gains, no abnormal organ changes; gene therapy, not protein injection. https://pubmed.ncbi.nlm.nih.gov/20368179/
- [2] Mendell JR, Sahenk Z, Malik V, et al. A phase 1/2a follistatin gene therapy trial for becker muscular dystrophy. Molecular Therapy, 2015. PMID 25322757. Six patients, AAV1.CMV.FS344; some six-minute-walk gains, reduced fibrosis, no serious adverse effects, mixed response. https://pubmed.ncbi.nlm.nih.gov/25322757/
- [3] Mendell JR, Sahenk Z, Al-Zaidy S, Rodino-Klapac LR, et al. Follistatin Gene Therapy for Sporadic Inclusion Body Myositis Improves Functional Outcomes. Molecular Therapy, 2017. PMID 28279643. Six treated versus eight untreated; six-minute walk improved 56.0 m/yr treated versus a 25.8 m/yr decline untreated, p = 0.01.
- [4] Reichel C, Gmeiner G, Thevis M. Detection of black market follistatin 344. Drug Testing and Analysis, 2019. PMID 31758732. Analytical method to detect black-market Follistatin 344; documents the unregulated gray-market supply.
- [F1] FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1s; objections to “sameness” claims and obscured compounding sources. FDA news release, March 3, 2026.
- [F2] FDA warning letter to Gram Peptides (representative of the March 31, 2026 peptide-seller letters), treating research-use-labeled peptide products as unapproved new drugs. FDA / CDER, March 31, 2026.
- [F8] Myostatin inhibitors including follistatin are prohibited at all times (hormone and metabolic modulators). WADA Prohibited List.
Written by Priya Moreno, reporter. Reporting from the sources cited above. Last reviewed June 2026.
Not professional medical advice. Speak with your healthcare provider before making a change.



